
Niger J Paed 2014; 41 (4): 345 - 349
ORIGINAL
Akodu SO
Exclusive breastfeeding practices
Njokanma OF
Disu EA
among women attending a private
Anga AL
health facility in Lagos, Nigeria
Kehinde OA
DOI:http://dx.doi.org/10.4314/njp.v41i4,11
Accepted: 31th May 2014
Abstract
Background: Exclusive
sively breastfed (3.6%).
breast feeding (EBF) is an effec-
No
association was found between
Akodu SO
(
)
tive tool of child survival. While
breastfeeding pattern and variables
Njokanma OF, Disu EA, Anga AL
many
mothers understand the
such
as gender of infants, place of
Kehinde OA
importance of breast
feeding,
delivery, maternal age, type of
Department of Paediatrics
some circumstances may hinder
delivery and number of antenatal
Lagos State University Teaching
visits. On the contrary there was
Hospital, Ikeja, Lagos, Nigeria
the practice.
Email: femiakodu@hotmail.com
Objective: To
determine the
pat-
an
association with following vari-
tern and factors influencing EBF
ables: birth order among mother
among women attending a private
siblings, prenatal and postnatal
health facility in Lagos, Nigeria.
feeding advice.
Methodology: One
hundred and
Conclusion: The
rate of
exclusive
twelve mothers with children aged
breast feeding among mothers for
twelve months or less were inter-
the recommended six months was
viewed through a questionnaire on
very low (3.6%). Antenatal and
their breastfeeding practices.
postnatal programmes that will
Results: At
the end
of second
encourage mothers to practice ex-
month, two-fifths of the babies
clusive breastfeeding should be
were still exclusively breastfed.
strengthened.
This dropped to one-fifth by the
end
of the fourth month. At the
Key words: Exclusive
breast feed-
end of six months, less than one-
ing, survival analysis, practice,
tenth of subjects were still exclu-
private hospital, mother
Introduction
the year 2003 2 .
According to the Nigerian Demographic
and Health Survey (NDHS), in 2008, 17% of children
Exclusive breastfeeding means that the infant receives
were exclusively breastfed for up-to four months, while
13% were exclusively breastfed up-to six months . This
2
only breast milk (either directly from the breast or ex-
pressed) and no other liquids or solids are given – not
data suggested a deteriorating situation; however, there
even water – with the exception of oral rehydration solu-
is
little or no information on the factors contributing to
tion, or drops/syrups of vitamins, minerals or medici-
this situation.
nes . The WHO recommends that infants should be ex-
1
clusively breastfed for the first six months of life to
The low proportion of women practicing EBF in most
achieve optimal growth, development and health.
2
developing countries has been attributed to various ma-
Thereafter, infants should receive nutritionally adequate
ternal and child factors including place of residence,
and
safe complementary foods, while continuing to
gender and age of the child, mother working outside
breastfeed for up to two years or more.
home, maternal age and educational level, access to
mass
media and economical status
9–11
Promotion of exclusive breastfeeding (EBF) has been a
.
Against the back-
cornerstone of public health measures to promote child
ground that the relative importance of these and similar
survival for several decades . EBF is associated with
3,4
factors may differ from one environment to another, the
reduced risks of diarrhoea–and pneumonia–related in-
current
study sought to assess exclusive breastfeeding
fant morbidity and mortality both developed and devel-
patterns among women attending a private health facility
oping world settings
5–
8
.
in
Lagos, Nigeria. Although several local studies have
been carried on the pattern of breast feeding among
Based on the WHO Global data on Infant and Young-
mothers, to the knowledge of the authors no study had
Child Feeding in Nigeria, 22.3% of children were exclu-
recruited mothers attending private hospitals. The im-
sively breastfed for less than four months, while 17.2%
portance of conducting the study in a private healthcare
were exclusively breastfed for less than six months, in
facility stems from the fact that clients of such facilities
346
are
often employed outside the home and are of rela-
First, at any time, subjects who are censored have same
tively high socioeconomic class.
survival prospects as those who continue to be followed.
Second, survival probabilities are the same for subjects
recruited early and late in the study. Third, the event
happens at the time specified. Survival probabilities,
Methodology
standard error, hazard rate and median survival time
were obtained. Log rank test for comparison of group
This was a descriptive cross-sectional study carried out
was also applied to compare EBF experiences of groups.
over a five–month period from March through July 2013
among women who brought their children to the immu-
EBF indicator was expressed as a dichotomous variable
nization unit at Isalu Hospitals Limited. Isalu Hospitals
with category “1” for EBF and category “0” for non-
Limited
is a private health facility located in Ogba,
EBF. This variable was examined against a set of inde-
Ikeja. Ogba is about five kilometres west of Ikeja, the
pendent variables (maternal and child characteristics) in
capital city of Lagos State. It is a densely populated area
order to determine the prevalence of EBF and factors
with a mixture of housing for high and low income earn-
associated with the duration of EBF. Log rank tests were
ers.
used to assess the significance of factors associated with
EBF and those with p < 0.05 were considered signifi-
Written and verbal informed consent was obtained from
cant.
respondents who brought their children to immunization
unit after explaining the purpose of the study. The tar-
gets were mothers with children aged less than twelve
months. Eligible subjects who consented were recruited
Results
consecutively.
Characteristics of the study subjects
Women were interviewed through a study proforma
The
characteristics of recruited mothers and their chil-
which included general information, socio-demographic
dren
are shown in Table 1. A total of 112 eligible
status, number of births, and duration of exclusive
mother-infant pairs were recruited for the study. Major-
breastfeeding, The duration of exclusive breastfeeding
ity
of the recruited mothers were above 30 years of age,
(in
months) here refers to the period from the first breast
have
tertiary educational status, are working mothers
milk
feed to the introduction of semi-solid or liquid food
and
belong to the upper socioeconomic strata. The most
supplements along with breastfeeding. Social classifica-
prevalent age group of the children was 9 – 11 months.
tion
was done using the scheme proposed by Oyedeji
12
Male and female children were nearly equally repre-
and subjects were classified into five classes (I – V) in
sented in the sample. Of the total births, 91.1% took
decreasing order of privilege. Socio-economic index
place at a private owned facility. The proportion of de-
scores (1 to 5) were awarded to each subject, based on
livery by caesarean section was 34.8%.
the occupational and educational levels of parents.
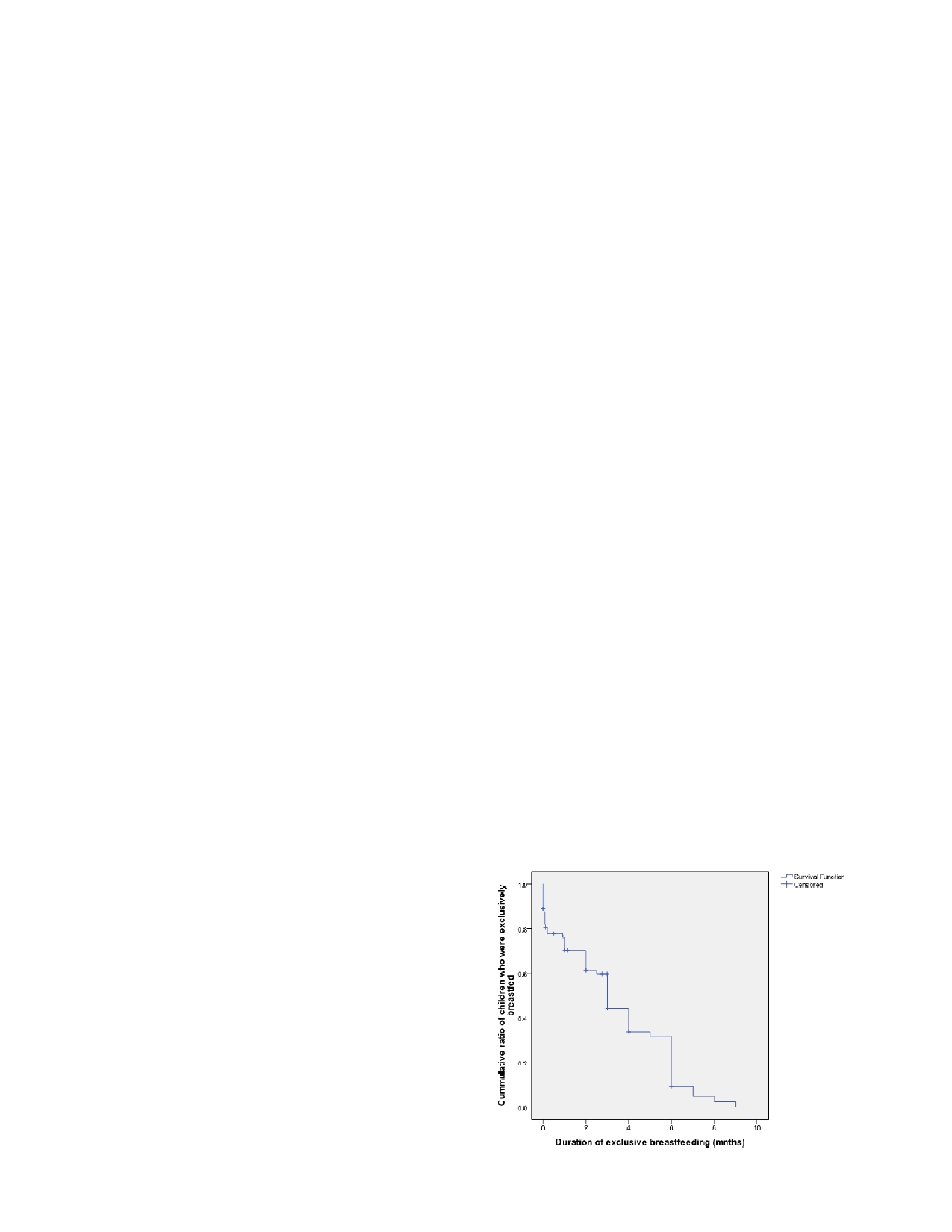
Cumulative probabilities for exclusive breast feeding
Data
were entered and analyzed using the Statistical
(EBF)
Package for Social Science (SPSS) 18.0 version. Those
women who were continuing EBF on the date of inter-
On
the basis of the life table technique, Figure 1 shows
view were considered censored cases and their duration
survival probability for duration of exclusive breastfeed-
of
EBF was recorded and treated as censored data, as it
ing
among study infants.
was
not known when they would discontinue EBF. They
contributed valuable information and were not to be
Fig 1: Survival
curve showing
survival probability for
duration
omitted from relevant aspects of the analysis. It would
of
exclusive breastfeeding
also
be wrong to treat the observed time at censoring as
exclusive breastfeeding termination time. A statistical
technique useful for such data is survival analysis. Life
table and the Kaplan Meier method was used to subdi-
13
vide
the period of observation into smaller time intervals
and
for each interval, all who had been observed at least
that
long were used to calculate the probability of a ter-
minal event occurring in that interval. The life table
technique allows us to consider children who were still
being breastfed at the time of interview of mothers, and
also
to know the proportion of children that remain be-
ing
breastfed by the end of each month of their life. So,
it
allows a longitudinal approach to the cross sectional
data
collected. The probabilities estimated from each of
the
intervals were then used to estimate the overall prob-
ability of the event occurring at different time points.
There were three assumptions for this methodology.

347
Table 1: Characteristics
of mothers
and children
Table 2: Cumulative
probabilities for
exclusive breast
feeding
Characteristic
N
%
using survival analysis
Gender of infant
Breast feeding
No
entering
No
of cumu-
No
of
Male
59
52.7
interval
the
interval
lative events
remaining
Female
53
47.3
(months)
cases
Age
of infant (months)
<3
40
35.7
0 –
1
112
22
65
3 –
5
13
11.6
1 –
2
65
28
45
6 –
8
4
3.6
2 –
3
45
38
27
9 –
11
46
41.1
3 –
4
27
44
18
No
response
9
8.0
4 –
5
18
45
17
Position of birth
5 –
6
17
57
4
1
46
41.1
>1
61
54.5
6 –
7
4
59
2
No
response
5
4.4
7 –
8
2
60
1
Place of delivery
8 -
9
1
61
0
Private hospital
102
91.1
Government hospital
10
8.9
Maternal age (years)
Factors associated with being exclusively breast fed
>30
73
65.2
21
– 30
39
34.8
Table 3 presents the survival analysis to investigate vari-
Mother’s education status
ables associated with being exclusively breastfed. The
Secondary
3
2.7
Tertiary
107
95.5
median duration for EBF was same for the female and
No
response
2
1.8
male babies (p = 0.757). The median duration of EBF
Father’s education status
was significantly longer among subjects of the second or
Secondary
1
0.9
higher birth order. The place of delivery, maternal age,
Tertiary
108
96.4
No
response
3
2.7
type of delivery and number of antenatal visits were not
Mother’s working status
associated with significant differences in median dura-
Housewife
2
1.8
tion of EBF (p > 0.05). On the contrary the report of
Working outside home
108
96.4
prenatal and postnatal feeding advice was associated
No
response
2
1.8
Socioeconomic status
with significantly longer median duration of EBF com-
Upper strata
106
94.6
pared with mother who reported no prenatal and postna-
Others
5
4.5
tal feeding advice (p < 0.05).
No
response
1
0.9
Type of delivery
Table 3: Survival
analysis of
factors associated
with exclu-
SVD
73
65.2
sively breastfeeding
C/S
39
34.8
Received prenatal feeding advice
Characteristic
No
of
No
of
Median duration of
Log
termi-
cen-
EBF
(months)
rank test
Yes
97
86.6
nal
sored
SE
(95% CI)
for
No
14
12.5
events
cases
com-
No
response
1
0.9
parison
of
group
Received postnatal feeding advice
Gender
0.757
Yes
71
63.4
Male
35
24
4.0
No
30
26.8
0.39 (3.25 – 4.76)
No
response
11
9.8
Female
26
27
4.0
0.75 (2.53 – 5.47)
Position of birth
1
26
20
3.0
0.012
Out of 112 women surveyed, 61 (54.5%) reported termi-
0.24 (2.53 – 3.47)
>1
33
28
6.0
nation of EBF on or before survey date (terminal event).
0.30 (5.41 – 6.60)
2.0
The remaining 51 (45.5%) cases were censored cases as
No
response
2
3
Place of delivery
0.510
they were still continuing EBF on the survey date. The
Private hospital
56
46
4.0
0.54 (2.94 – 5.06)
overall exclusive breastfeeding rate was 42.9 percent.
Government hospital
5
5
3.0
Maternal age (years)
0.22 (2.57 – 3.43)
Table 2 show the cumulative probabilities for EBF using
>30
survival analysis. In relation to exclusive breastfeeding,
42
31
3.0
0.671
21
– 30
0.41 (2.20 – 3.80)
it
was observed that this was not a universal practice
Type of delivery
19
20
4.0
0.64 (2.75 – 5.25)
immediately after birth as 22 (19.7%) had formula feed
C/S
17
22
6.0
introduced. The maximum numbers of babies who
SVD
1.51 (3.05 – 8.96)
44
29
4.0
0.767
stopped EBF did so during first month of age interval,
Number of antenatal visits
0.43 (3.17 – 4.83)
1 –
3
4
3
4.0
which are 22 babies. By the end of second month, forty-
2.49 (0.00 – 8.89)
five of the recruited children were still exclusively
More than 3
55
46
4.0
0.38 (3.26 – 4.74)
breastfed, which further dropped to eighteen by the end
No
response
2
2
0.00
0.766
4.0
of
the fourth month. At the end of six months, four of
Received prenatal feeding advice
0.51 (3.01 – 4.99)
the recruited children were still exclusively breastfed.
Yes
51
46
1.0
0.44 (0.13 – 1.89)
The median length of exclusive breastfeeding (age in
No
9
5
2.0
which half of the children received only the mother’s
No
response
1
0
4.0
0.001
milk) was found to be three months (with 95% confi-
Received postnatal feeding
0.49 (3.05 – 4.95)
advice
3.0
dence interval 2.61 – 3.40).The overall mean duration of
Yes
38
33
0.66 (1.72 – 4.29)
No
2.0
exclusive breast feeding among respondents was 3.82
No
response
17
13
0.69 (0.65 – 3.35)
months (with 95% confidence interval 3.25 – 4.39).
6
5
0.003
348
Discussion
encourage mothers to practice EBF of subsequent babies
while negative experiences would do the opposite.
The
survival analysis method was used to analyze data
Again, personal motivation might influence even a
from 112 mothers. The median duration of EBF in the
mother who had unpleasant experiences the first time to
current study (three months) was lower than five months
attempt EBF the next time around. The extent to which
reported by Chudasamaa et al among 498 mothers in-
14
previous experiences and motivation play a role in EBF
fant pairs in South Gujarat region of India, five years
will therefore differ from one cohort of mothers to an-
ago. On the contrary, the median duration of EBF re-
other.
ported in the current study is similar to three months
reported by Setegnet al
15
among 608 mothers in Goba
In
the present study, prenatal EBF plan by way of prena-
district, Southeast Ethiopia. However, it is of interest to
tal feeding advice was found to be associated with
note that the median duration of EBF reported in the
longer duration of EBF. This finding was in agreement
present study was higher than the reported national dura-
with a study conducted among mothers in Bahir Dar
City, Northwest Ethiopia . This might be attributable to
21
tion of half a month but less than seven months reported
in
Southwest Nigeria by the National Population Com-
planning, increased preparedness, and commitment to
mission .
16
achieve EBF. Similarly, the postnatal feeding advice
was associated with longer duration of EBF.
It
was observed in the present study that the month dur-
ing
which the highest number of mothers discontinued
EBF
was at the end of first month. The explanation for
this
finding might be the effect of work resumption.
Conclusion
Usually working mothers in Nigeria are allowed 12
weeks of maternity leave which equals approximately
In
conclusion, this study identified birth order, prenatal
three months. Under these circumstances, mothers are
feeding advice, and postnatal feeding to be associated
prompted to resort to the supplementation of infant for-
with exclusive breastfeeding and that practice of exclu-
mula before three months so that their infants get accus-
sive breast feeding among mothers declined to below
tomed to bottle feeding. Maternal fatigue and the diffi-
20% by the end of four months when they may have
culty in juggling the demands of work and breastfeeding
resumed work. Health workers in private health facilities
may also contribute to this issue. The finding indicates
should play a more prominent role in providing informa-
that the passing and enforcement of legislation that sup-
tion about exclusive breastfeeding to mothers before and
ports working mothers who want to breast-feed exclu-
after delivery.
sively should be a priority. Such legislation includes
initiating breastfeeding-friendly work environments, as
Authors’ contributions
well as the extension of maternity leave to encourage
Akodu SO: Conception, Data collection, Analysis,
mothers to exclusively breastfeed their babies to im-
Manuscript writing.
prove child health outcomes.
Njokanma OF: Conception, Data collection, analysis
Disu EA: Conception
Exclusive breastfeeding (EBF) experiences of two
Anga AL: Conception, Data collection
groups of infants namely, those of first birth order and
Kehinde OA: Conception, Data collection
those of second or higher birth order were determined.
Conflict of interest: None
The median duration of EBF was observed to be signifi-
Funding: None
cantly higher among infants with second or more order.
This observation might be related to previous breast
feeding experiences of their mothers. The effect of
mother parity on duration of EBF is still a matter of con-
troversy. While some authors have reported that lower
Acknowledgement
parity is associated with longer duration EBF others
17
have documented that higher parity leads to longer dura-
We
thank all the mothers who participated in the study
.
In another study , it was asserted that
20
tion of EBF
18,
19
as
well as the Medical Director and staff of Isalu
parity had no significant influence on duration of EBF.
Hospitals Limited, Ogba, Lagos.
It
would appear that positive personal experiences would
References
1.
WHO. Indicators for Accessing
2.
Agbo HA, Envuladu EA, Adams
3.
Jones G, Steketee RW, Black RE,
Breastfeeding Practices. WHO/
HS,
et al. Barriers and facilitators
Bhutta ZA, Morris SS. The Bella-
CDD/ SER/911. Geneva: World
to
the practice of exclusiveBreast
gio
Child Survival Study - How
Health Organization 1991.
feeding among working class
many child deaths can we prevent
mothers: A studyof female resident
this year? Lancet
2003; 362:
65 –
doctors
in tertiary health institu-
71.
tionsin Plateau State. J
Med Res
4.
Jelliffe DB, Jelliffe EF. Human
2013; 2: 112 – 6.
milk in the modern world. New
York: Oxford University Press
1978.

349
5.
Quigley MA, Kelly YJ, Sacker A.
11.
Shirima R, Greiner T, Kylberg E,
17.
Sloan S, Sneddon H, Stewart M,
Breastfeeding and hospitalization
et
al. Exclusive breastfeeding is
Iwaniec D. “Breast is best? Rea-
for
diarrheal and respiratory infec-
rarely
practised in rural and urban
sons why mothers decide to
tion in the United Kingdom Mil-
Morogoro. Tanzania Public Health
breastfeed or bottlefeed their ba-
lennium Cohort Study. Pediatrics
Nutrition 2000; 4(2): 147-54.
bies and factors influencing the
2007; 119: 837 - 42.
12.
Oyedeji GA. Socio-economic and
duration of breastfeeding,”Child
6.
Victora CG, Smith PG, Vaughan
cultural background of hospital-
Care Pract 2006; 12: 283 – 97 ,
JP,
et al. Evidence for protection
ized children in Ilesha. Nig J
Pae-
18.
Wojcicki JM, “Maternal prepreg-
by
breast-feeding against infant
diatr 1985; 12: 111 - 7.
nancy body mass index and initia-
deaths from infectious diseases in
13.
Allison PD. Survival analysis
tion and duration of breastfeeding:
Brazil. Lancet
1987; 2:
319 –
22.
using SAS: A practical guide.
a
review of the literature,”J
2
ed. Carry: SAS Institute Inc;
nd
7.
Popkin BM, Adiar L, Akin J,
Women Health 2011; 20: 341 – 7.
Black R, Briscoe J, Fleiger W.
2010.
19.
Abada TSJ, Trovato F, Lalu N.
Breast feeding and diarrheal mor-
14.
Chudasamaa RK, Patelb PC, Kav-
“Determinants
of breastfeeding in
bidity. Pediatrics
1990; 86:
874 –
ishwarc
AB. Determinants of Ex-
the
Philippines: a survival analy-
9.
clusive Breastfeeding in South
sis,”SocSci
Med 2001;
52: 71
–
8.
Arifeen S, Black RE, Antelman G,
Gujarat Region of India. J
Clin
81,
et
al. Exclusive Breastfeeding
Med Res 2009;1:102-8
20.
Ekstrom A, Widstrom A, Nissen
Reduces Acute Respiratory Infec-
15.
SetegnT, Belachew T, Gerbaba M,
E.
“Duration of breastfeeding in
tion and Diarrhea Deaths Among
Deribe K, Deribew A, Biadgilign
Swedish primiparousandmultipa-
Infants in Dhaka Slums. Pediatrics
S.
Factors associated with exclu-
rous women,”J
Hum Lact
2003;
2001; 08; e67. Available from:
sive breastfeeding practices among
19: 172–8.
http://www.pediatricsdigest.mobi/
mothers in Goba district, south
21.
Seid AM, Yesuf ME, Koye DN.:
content/108/4/e67.full.pdf+html
east Ethiopia: a cross-sectional
Prevalence of Exclusive Breast-
9.
Ssenyonga R, Muwonge R, Nan-
study. Int
Breastfeed J
2012; 7:17
feeding Practices and associated
kya
I. Towards a Better Under-
- 25
factors among mothers in Bahir
standing of Exclusive Breastfeed-
16.
National Population Commission
Dar
city, Northwest Ethiopia: a
ing
in the Era of HIV/AIDS: A
(NPC) Nigeria and ICF Macro:
community based cross-sectional
Study of Prevalence and Factors
Nigeria Demographic and Health
study. Int
Breastfeed J
2013; 8:14
Associated with Exclusive Breast-
Survey 2008 Calverton, Maryland,
- 22.
feeding from Birth, in Rakai,
USA:NPC and ICF Macro
Uganda .
J Trop
Pediatr 2004;
50
2009.Available from: http://
(6): 348 - 53.
www.population.gov.ng/images/
10.
Haider J, Kloos H, Haile Mariam
Nigeria%20DHS%202008%
D,
et al. Food and Nutrition. In:
20Final%20Report.pdf.
Berhane Y, Haile Mariam D,
Kloos H, Eds. The Epidemiology
and
Ecology of Health and Dis-
eases in Ethiopia Addis Ababa,
Ethiopia: Shama Books 2006.